|
|
|
|
Jeffrey Dach, M.D. NewsLetter
Blood Pressure Pills for Hypertension, When to Treat?
by Jeffrey Dach MD
__________________________________________
Dear Friend or Colleague
A good friend, age 60, has a mild hypertension, 147 systolic, and accordingly takes blood pressure pills. The current guideline recommends treatment for blood pressure above 140 systolic, regardless of age, usually with a “water pill” called a thiazide diuretic(1). My friend asks me, does he need to take these blood pressure pills forever?
Blood Pressure 101, the Real Story
As we age, we all develop "hardening of the arteries", also called atherosclerotic vascular disease. This involves the gradual loss of flexibility and increased stiffeness of the arterial walls from loss of elastin fibers as we age. This process also involves a more serious caking up of plaque inside the arteries which can block blood flow and cause a heart attack or stroke.
Mechanical Stress from Pulsations Produces Damage
Our hearts beat about 80 times per minutes at rest, and each heart beat produces a pulsatile wave of pressure which expands the arterial wall. These pulsatile waves produce mechanical stress which cause small cracks at weak points where the arteries divide. The body must repair these cracks, and the repair mechanism involves deposition of cholesterol plaque to seal these small cracks and prevent leakage. The final result of the repair process is the plaque buildup which blocks blood flow causing heart attacks and strokes. Sometimes the repair process involves inflammation which causes more damage to the lining of the artery.
A Lower Blood Pressure Reduces Mechanical Stress on the Arteries
Reducing the blood pressure obviously reduces the mechanical stress on the arteries, and thereby reduces the risk of heart attack and stroke. The real question is, "what blood pressure level requires treatment?", and "what is the optimal target area for the lowered blood pressure?" A blood pressure brought too low with pills leads to dizziness and fainting, so too low is not good either.
Blood Pressure Normally Rises with Age
The blood pressure increases gradually with age, a normal consequence of aging, but the guidelines ignore this, and use the same number, 140 as a treatment threshold for all ages, and genders. (22) Why is this?
The Famous Framingham Study, the Basis for the BP Guideline
The blood pressure treatment guideline is based on the famous Framingham Study which showed the benefits of blood pressure reduction. The 18 year Framingham Blood Pressure study found increased risk of heart disease and death in people with blood pressure 140 to 160, and even more risk above 160. (NEJM, Levy) (2) (4) (5) (6) (7) (8).
Discrepancy Between Raw Data and Computer Smoothed Data:
Let's examine the original data from the study in Figure 1 (below). Here is the Framingham Study Data with computer smoothing as published in the medical journals. Note the smooth gradual line of increasing mortality as blood pressure goes up between 140 and 160. This is called the Linear Model.(from Port, Lancet)(17)(18) Figure 1 below.
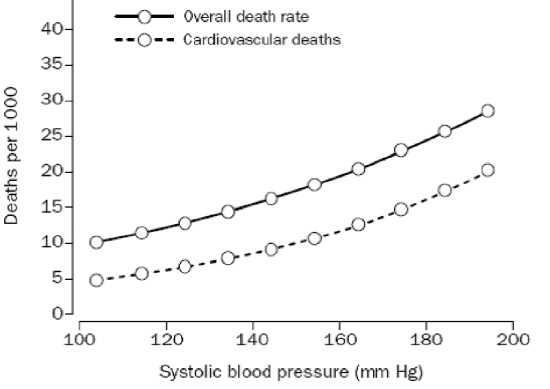
Figure 1.
Next in Figure 2 (below), here is the original Framingham RAW Data before computer smoothing. Notice the mortality rate is fairly constant at 15 deaths per 1000 until a blood pressure of 160 is exceeded. The relationship is NOT linear. (from Port, Lancet)(17)(18) These two charts, Figure 1 and Figure 2, are quite different.
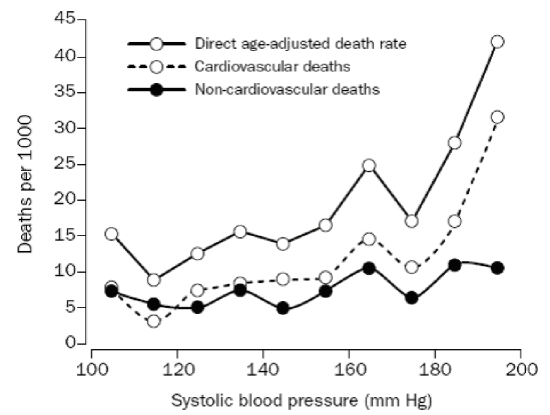
Figure 2.
Notice that the raw data in Figure 2 does not support the Linear Model.
Doctor Port introduces a new model which takes into account age and gender. The mortality risk increases steadily with blood pressures that exceed a threshold based on sex and age. The threshold blood pressure formula is 110 + (2/3) (age) for a man aged 45-74, and 104 +(5/6) age for a woman aged 45-74. Here is the Lancet chart for the blood pressure thresholds, showing treatment thresholds based on age and gender. (17) (18)
Age......Male BP Threshold....Female BP Threshold 70th percentile
45..........139.........................142
50..........143.........................146
55..........147.........................150
60..........150.........................154
65..........153.........................158
70..........157.........................162
According to this chart, a blood pressure of 147 in a 60 year old man does not require treatment with “water pills”. Blood pressure goes up with age, and this is normal.
Before you run to your doctor with a print out of this newsletter, please be aware of the response by Dr. Lenfant, Director National Heart, Lung, and Blood Institute (NHLBI), the agency which funded Dr. Port’s report. Dr. Lenfant outright rejected Dr. Port’s non-linear model, and he restates his belief the relationship between mortality and blood pressure is a clear linear one. (9)
Here is what Dr. Lenfant says, “A study funded by the National Heart, Lung, and Blood Institute (NHLBI) and published in the January 15 issue of the Lancet (by Port) challenges [us] by asserting that the relationship between systolic blood pressure and mortality is not "continuous and graded." After careful review of this study, the NHLBI finds that it does not offer a basis for changing the current hypertension guidelines….We attach great value to new scientific findings and our careful review of Dr. Port's paper finds his analysis thought provoking. However, we would not recommend a change in the guidelines based on one epidemiological analysis….The totality of evidence found a clear linear relationship between systolic blood pressure, diastolic blood pressure and deaths.”
Perhaps Dr. Lenfant didn’t actually look at figure 2 raw data which clearly shows it is non-linear.
Dr. Lewiston published a rebuttal in Lancet 2002 which says ” Throughout middle and old age, usual blood pressure is strongly and directly related to vascular (and overall) mortality, without any evidence of a threshold down to at least 115/75 mm Hg” (12). Dr. Lewiston didn’t look at raw data figure 2, either.
Jan Basile, MD, Walter A. Brzezinski, MD published a
rebuttal in the Journal of Clinical Hypertension J Clin Hypertens 2(4):290-294, 2000. which says that the Port paper did not evaluate morbidity, (non-fatal strokes and heart attacks) which the SHEP study examined, and showed considerable reduction in morbidity by reducing systolic pressure. (15). They argued that the reduction in stroke morbidity in the SHEP study justifies treatment with blood pressure pills for the 140-160 range. This discussion can be found at the angrydoc blog (14).
The problem with this reasoning is the SHEP study patients all started with blood pressures above 160, and does not address the below 160 question asked by Port. The Shep data showed a reduction of 5 years stroke rate from 8.2 to 5.2 per cent. However the average blood pressure was 170, with all patients above 160 at the start. There is no question that BP’s above 160 require treatment, our question pertains to the 140 to 160 range which showed no increased mortality in the Framingham raw data. "No randomized trial has ever demonstrated any reduction in risk of either overall or cardiovascular death by reducing systolic blood pressure from the thresholds in the above chart by Dr. Port to below 140 mm HG"(18).
Three Factors at Work
What is the risk of stroke and heart attack at any particular blood pressure? Is lower better and how low is better? Perhaps the use of blood pressure to assess CV disease risk is too simplistic. The causes of arterial disease are more complicated, with at least three factors at work.
First Factor is Mechanical Stress
The first factor is the mechanical stress on the artery wall represented by the pressure. This pressure wave is pulsatile, and has a waveform which is more complex than a simple blood pressure number. The second factor is the intrinsic strength of the arterial wall which is made of collagen. The third factor is the vigor of the reparative mechanism mounted as a defense against the small cracks in the wall from mechanical stress which may cause an inflamatory response inside the arterial wall.
Arterial Stiffness
Arterial stiffness increases with age, requiring more pressure to perfuse the arterial system than the younger, more elastic arterial tree. This "arterial stiffness" can be studied with various techniques such as ultrasound of carotid artery thickness, the pulse pressure and the pulse wave form, and these techniques are all excellent indicators of cardiovascular disease risk and strong predictors of stroke, and actually may be more representative of mechanical stress on the arterial wall than simple blood pressure measurement. (24) (25)
Second Factor is Arterial Strength
The second factor is the intrinsic strength of the arterial wall which is made of the protein called collagen. For example, vitamin C deficiency is associated with poor collagen formation and increased risk of stroke as discussed in a previous newsletter (27). Blood pressure pills do nothing to improve the strength of the arterial system, on the other hand, vitamin C does.
The trace mineral Copper is required as a cofactor for elastin production which allows the arteries to be flexible and elastic. Copper deficieny is associated with weakening in the wall and bubble formation in the arteries, called aneurysms, caused by lack of elastin (26) The third factor, inflammation inside the artery as a repair mechanism can be addressed with options discussed on my web site at this page
Complete Evaluation is More than a Simple Blood Pressure
A more complete vascular evaluation includes an ultrasound of the carotid arteries to measure wall thickness, an aortic ultrasound to screen for aneurysm, and measurement of the pulse pressure (this is the difference between systolic and diastolic pressures). A knowledge of the medical history and pre-existing risk factors such as smoking and diabetes is also important. After reviewing all this information, an informed decision can be made to treat or not to treat patients with blood pressures below 160.
Linear or Nonlinear Model is a Personal Choice
In a healthy adult with no other risk factors, and a blood pressure below 160, the Framingham Study raw data clearly shows no mortality risk. Therefore, following the guidelines published in Lancet by Port is a valid personal choice.
The current blood pressure treatment guidelines are based on deceptive data smoothing on the Framingham data set, resulting in lower treatment thresholds which translate into extra billions of dollars for the drug companies. Should you accept the “Linear Model” or the NonLinear model? That is an indivisual decision that is up to you. After all, its your blood pressure.
More information on lowering your blood pressure naturally without drugs can be found at my web site at this page.
Thanks to Joel Kauffman PhD for chapter 4 in his book, Malignant Medical Myths which brought this information to my attention.(10)
Did you find this newsletter interesting? Feel free to email this to a friend with the button on the bar at the bottom of the page.
Regards,
Jeffrey Dach, M.D.
BLOG
TrueMedMD
Newsletter
4700 Sheridan, Suite T.
Hollywood Florida, 33021
954 983 1443
References:
(1) Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, Jones DW, Materson BJ, Oparil S, Wright JT Jr, Roccella EJ. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension 2003 Dec;42(6):1206-52. [386 references]
(2)
Framingham Heart Study
(3)
Framingham Study
(4) list of publications from the Framingham heart study
(5) NIH Framingham study web site
(6)1288 publications from the Framingham data
(7) hypertension online, PowerPoint Slides of all the major studies
(8)
NEJM Framingham study by Levy
(9)
Statement from Claude Lenfant, M.D., NHLBI Director, on Systolic Blood Pressure, Deaths, and Treatment Guidelines
(10) "Malignant Medical Myths" by Joel Kaufman, PhD, page 105 to 129, Myth 4.
(11) list of 150 blood pressure pills
(12) Lewington S, et al.;Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002 Dec 14;360(9349):1903-13.
This Confirms Linear Model “INTERPRETATION: Throughout middle and old age, usual blood pressure is strongly and directly related to vascular (and overall) mortality, without any evidence of a threshold down to at least 115/75 mm Hg.”
(13) The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report. JAMA. 2003 May 21;289(19):2560-72. Confirms Linear Model.
(14) Vol. 265 No. 24, June 26, 1991 JAMA Linear Model
(15) SHEP Cooperative Research Group. Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension: final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA. 1991;65:3255–3264.
CONCLUSION. In persons aged 60 years and over with isolated systolic hypertension, antihypertensive stepped-care drug treatment ...reduced the incidence of total stroke by 36%, with 5-year absolute benefit of 30 events per 1000 participants. Major cardiovascular events were reduced, with 5-year absolute benefit of 55 events per 1000.
(16) FRAMINGHAM HEART STUDY.NEJM Volume 329:1912-1917 December 23, 1993 Number 26 The Natural History of Borderline Isolated Systolic Hypertension Alex Sagie, Martin G. Larson, and Daniel Levy
(17) Lancet. 2000 Jan 15;355(9199):175-80. Systolic blood pressure and mortality. Port S, Demer L, Jennrich R, Walter D, Garfinkel A. (Port article #1)
(18) Full Text
(18a) Abstract, Lancet. 2000 Jan 15;355(9199):175-80. Systolic blood pressure and mortality. Port S, Demer L, Jennrich R, Walter D, Garfinkel A.
(19)
angry doc blog
(20) hypertension online slides
(21) assessment of arterial stiffness in clinical practice
(22) Circulation. 1997;96:308-315.Hemodynamic Patterns of Age-Related Changes in Blood Pressure The Framingham Heart Study Stanley S. Franklin, MD; William Gustin, IV, BS; Nathan D. Wong, PhD; Martin G. Larson, ScD; Michael A. Weber, MD; William B. Kannel, MD; ; Daniel Levy, MD. Framingham study which shows BP increases with age.
(24) Circulation. 1999;100:951-957. Common Carotid Intima-Media Thickness and Arterial Stiffness, Indicators of Cardiovascular Risk in High-Risk Patients The SMART Study (Second Manifestations of ARTerial disease) Petra C. G. Simons, MD, PhD; Ale Algra, MD, PhD; Michiel L. Bots, MD, PhD; Diederick E. Grobbee, MD, PhD; Yolanda van der Graaf, MD, PhD; for the SMART Study Group
(25)
(Hypertension. 1999;34:375-380.) Isolated Systolic Hypertension
Prognostic Information Provided by Pulse Pressure Michael J. Domanski; Barry R. Davis; Marc A. Pfeffer; Mark Kastantin; Gary F. Mitchell
Abstract—Increased arterial stiffness results in increased characteristic impedance of the aorta and increased pulse wave velocity, which increases systolic and pulse pressures. An association between increased pulse pressure and adverse cardiovascular events has been found in normotensive and hypertensive patient populations. Increased pulse pressure has also been associated with thickening of the carotid intima and media. However, the relationship between pulse pressure and stroke has not previously been evaluated. In this study, we examined the hypothesis that pulse pressure is an independent predictor of stroke in elderly patients with systolic hypertension entered in the Systolic Hypertension in the Elderly Program. Differences in baseline characteristics were examined by tertiles of pulse pressure. The independent prognostic value of pulse pressure and mean arterial pressure for predicting either stroke or total mortality was assessed with Cox proportional hazards models that included pulse pressure, mean arterial pressure, and other variables that were significant on univariate analysis. This analysis demonstrated an 11% increase in stroke risk and a 16% increase in risk of all-cause mortality for each 10-mm Hg increase in pulse pressure. Each 10-mm Hg increase in mean arterial pressure was independently associated with a 20% increase in the risk of stroke and a 14% increase in the risk of all-cause mortality. These data provide strong evidence of an association of increased conduit vessel stiffness, as indicated by increased pulse pressure, with stroke and total mortality, independent of the effects of mean arterial pressure, in elderly patients with isolated systolic hypertension.
(26) Arch Surg. 1982 Sep;117(9):1212-3. Decreased hepatic copper levels. A possible chemical marker for the pathogenesis of aortic aneurysms in man.Tilson MD. Copper is a cofactor for elastin production. Copper is needed for the proper function of the enzyme lysyl oxidase, which is required in the crosslinking of collagen and elastin.
(27) Vitamin C and Stroke Prevention by Jeffrey Dach MD.
|
|
|
|
|
Jeffrey Dach, M.D. TrueMedMD
Catalog of NewsLetters
_______________________________________________________________
Enter your email address to subscribe to newsletter.
Your email is safe and will never be shared.
_______________________________________________________________
|
(1)
My Vitamins Are Killing Me by Jeffrey Dach MD !!!
(2)
Stroke Prevention and Vitamin C by Jeffrey Dach MD
(3)
Testosterone Risks and Benefits by Jeffrey Dach MD
(4)
Medical School Days and SSRI Research by Jeffrey Dach MD
(5)
Iodine and Breast Cancer Prevention by Jeffrey Dach MD
(6)
Hypothyroidism Part One by Jeffrey Dach MD
(7)
Hypothyroidism Part Two Thryroflex by Jeffrey Dach MD
(8)
Guard Your Daughter from Gardisil, Virginia Tech Rampage Seung-Hui Cho by
Jeffrey Dach MD
(9) Orthomolecular Medicine Meeting in Toronto 2007 by Jeffrey Dach
MD
(10) B12 Deficiency by Jeffrey Dach MD
(11) Rachel Carson and Silent Spring by Jeffrey Dach MD
(12) Vitamin D Deficiency by Jeffrey Dach MD
(13) Andrew Weil AARP, and Human Growth Hormone HGH by Jeffrey Dach MD
(14) Michael Moore's SICKO by Jeffrey Dach MD
_______________________________________________________________
Catalog of Articles Published on Hank Barnes World,
You Bet Your Life, by Jeffrey Dach MD
_______________________________________________________________
(1)
Lipitor and "The Dracula of Modern Technology" by Jeffrey Dach MD
(2)
Osteoporosis, Bisphosphonate Drugs and Toulouse Lautrec by Jeffrey Dach
MD
(3)
Prozac, Paxil and SSRI Drugs - Part One by Jeffrey Dach MD
(4)
Prozac, Paxil and SSRI Drugs - Part Two by Jeffrey Dach MD
(5)
Max Essex and Virological Failure in the NEJM by Jeffrey Dach MD
(6)
The Origins of HIV by Jeffrey Dach MD
A Medical Article that I Published in 1980:
(7)
Dach J, Patel N, Patel S, Petasnick J. Peritoneal mesothelioma: CT,
sonography, and gallium-67 scan. AJR Am J Roentgenol. 1980 Sep;135(3):614
Jeffrey Dach, M.D.
Member of the Board of the American Academy of Anti-Aging Medicine
Board Certified by the American Board of Radiology
4700 Sheridan, Suite T
Hollywood Fl 33021
office phone 954-983-1443
_______________________________________________________________
Don't forget to visit
my web site for more information, and we you might like to attend
one of our free seminars on Wednesday Nights. Please call for
reservations for the seminar, though.
Do you have a testimonial, or a question for the newsletter? Send it in
via email reply.
Sincerely Yours
Jeffrey Dach, M.D.
4700 Sheridan Suite T.
Hollywood, Fl 33021
954-983-1443
_______________________________________________________________
Dr. Dach is Board Certified by the American Board of Radiology and a
member of the Board of the American Academy of Anti-Aging Medicine.
He has 25 years experience in the Memorial Hospital System as an
interventional radiologist. His current practice focuses on Bio-identical
hormone supplementation for men and women, menopause, andropause, HGH,
testosterone, natural thyroid and the use of natural substances rather
than drugs in the appropriate setting.
Conflict of Interest Disclaimer: We receive no money from the
pharmaceutical industry or from the NIH. We do not sell any products to
the public at large. We do however, make available selected nutritional
supplements to our office clients at a small markup to cover our costs.
If this email is sent to you in error, please accept our apology, and
simply remove your email from the list with the unsubscribe button on the
bar below this text. Sorry for the inconvenience.
(c) 2007 all right reserved Jeffrey Dach MD
disclaimer
|
|
|
|